
Spondylolisthesis & Spondylosis
Overview
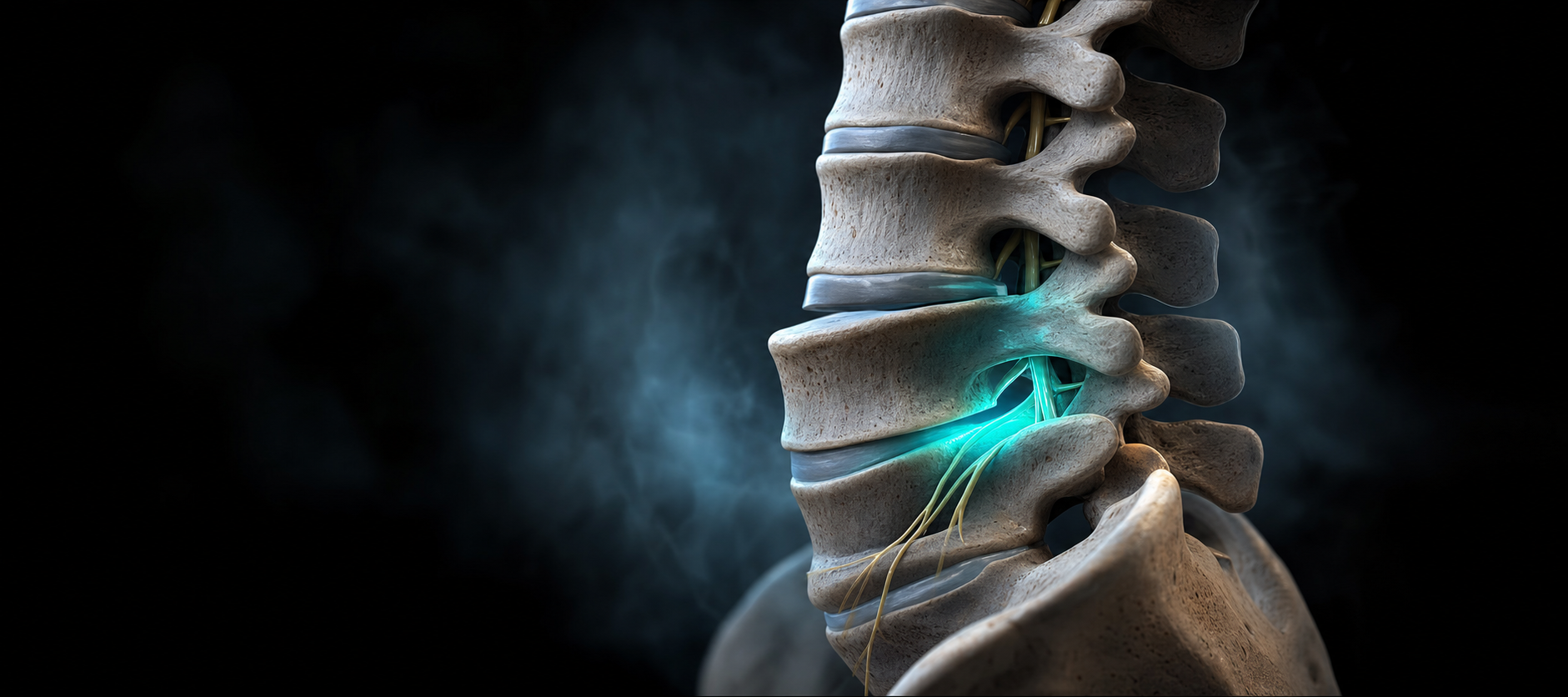
Spondylolisthesis and spondylosis are two distinct but often co-occurring degenerative spinal conditions. Spondylolisthesis refers to the forward (or occasionally backward) slippage of one vertebra over the one below it, creating instability and potential nerve compression. Spondylosis is a broader term for age-related degenerative changes throughout the spine — including disc degeneration, bone spur formation, and facet arthritis — that collectively narrow the spinal canal and foramina. Together, these conditions are among the most common sources of chronic spinal pain in adults over 40.
Common Symptoms
•Chronic lower back or neck pain that may be dull or sharp
•Leg pain, numbness, or weakness (if nerve roots are compressed)
•Stiffness and reduced range of spinal motion
•Pain that worsens with prolonged activity and improves with rest
•A feeling of spinal instability or "slipping" with movement
•Neurogenic claudication — pain and cramping in the legs with walking (when stenosis co-exists)
Common Causes
•Age-related disc degeneration reducing disc height and stability
•Defect or fracture in the pars interarticularis of the vertebra (isthmic spondylolisthesis)
•Degenerative arthritis destabilizing the facet joints (degenerative spondylolisthesis)
•Congenital vertebral anomalies
•High-impact sports or repetitive hyperextension activities
•Prior spinal injury or surgery altering biomechanics
Who May Benefit from Treatment
Adults experiencing chronic back pain with or without leg symptoms — particularly those with imaging showing vertebral slippage or significant degenerative changes — benefit from Echo PMR's individualized management. Patients seeking to avoid surgery or those with low-grade (Grade I–II) spondylolisthesis are excellent nonsurgical candidates.
Treatment Options at Echo PMR
•Epidural steroid injections — relieve nerve root inflammation caused by foraminal or canal compression from slippage or bone spurs
•Medial branch blocks and radiofrequency ablation (RFA) — target the facet arthritis component driving segmental pain
•SI joint injections — address secondary SI joint overload from altered lumbar mechanics
•Physical therapy — lumbar stabilization programs specifically designed to support the unstable segment and reduce shear forces
•Medication management — anti-inflammatory agents, muscle relaxants, and neuropathic medications as clinically indicated
•Spinal cord stimulation — for patients with refractory neurogenic leg pain
Recovery Expectations
Many patients with low-grade spondylolisthesis achieve excellent symptom control with a combination of spinal injections and a structured stabilization therapy program. Pain relief from RFA can last 12–24 months, and repeated procedures are safe and effective. The goal of treatment is to keep patients functional, comfortable, and independent — avoiding or delaying surgery whenever possible.
When to Seek Care
If you have been diagnosed with spondylolisthesis or spondylosis and your pain is interfering with work, sleep, or daily life, contact Echo PMR for a comprehensive evaluation. Early, consistent management produces better long-term outcomes and helps preserve spinal stability.