
Percutaneous Disc Decompression
What Is Percutaneous Disc Decompression?
Percutaneous disc decompression (PDD) is a minimally invasive outpatient procedure that reduces internal disc pressure by removing a small amount of disc material from the nucleus pulposus — the soft inner core of a spinal disc. By decreasing volume and pressure within the disc, the procedure relieves tension on surrounding nerve roots without the need for open spinal surgery. It is best suited for patients with contained disc herniations causing nerve-related pain such as sciatica.
How It Works
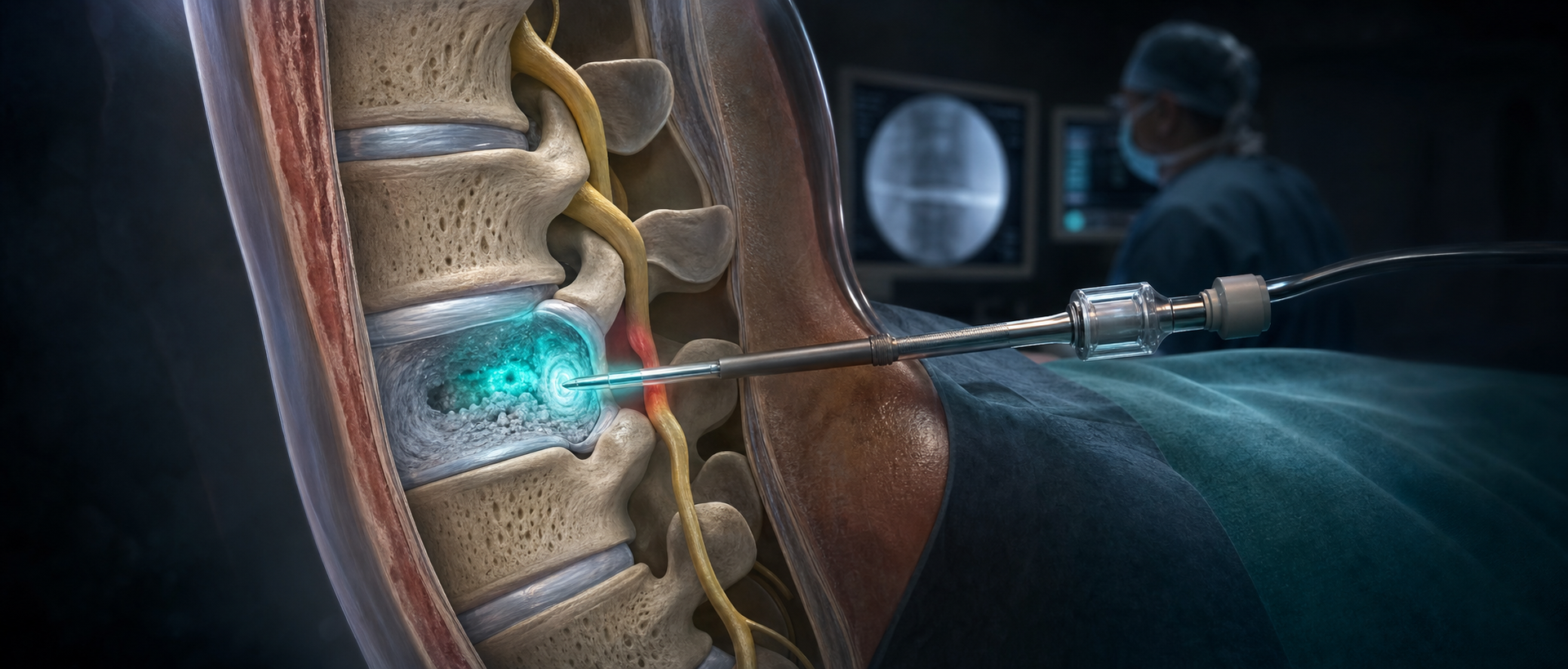
A needle or probe is precisely guided through the skin and into the center of the herniated disc under fluoroscopic imaging. Depending on the technique used — which may include mechanical removal, laser energy, or radiofrequency-based plasma technology (nucleoplasty) — a small portion of nucleus material is removed or vaporized. Reducing internal disc volume decreases the bulge pressing on nearby nerves, providing decompression of the neural structures.
•Minimally invasive: No incision, no stitches — only a small needle entry point
•Image guidance: Fluoroscopy ensures the probe is precisely placed in the disc nucleus
•Pressure reduction: Removal of a small disc volume significantly reduces intradiscal pressure
•Outpatient: Performed in an ambulatory procedure center; no hospital stay required
What to Expect During the Procedure
•Preparation: IV access is established; the skin is sterilized and numbed with local anesthetic
•Duration: 30–45 minutes depending on the number of levels treated
•Guidance: Continuous fluoroscopy throughout the procedure
•Anesthesia: Local anesthetic with IV sedation for comfort; general anesthesia is not required
•Same-day recovery: Most patients go home within 1–2 hours; activity restrictions apply for 1–2 weeks
Conditions Treated
•Contained lumbar disc herniation with sciatica
•Cervical disc herniation with arm pain (cervical radiculopathy)
•Discogenic pain confirmed by discography
•Lumbar radiculopathy unresponsive to epidural steroid injections
•Early-stage disc degeneration with nerve compression
•Chronic back and leg pain from disc bulge
Who Is a Good Candidate?
Ideal candidates have a contained disc herniation (the outer disc wall is intact) with radicular symptoms — such as sciatica — that correlates with imaging findings and has not responded to at least 6 weeks of conservative treatment including physical therapy and injections. Patients who wish to avoid or delay open surgery are particularly well-suited for this approach.
Recovery & Results
Most patients return to light activity within a few days and normal activity within 2–4 weeks. Nerve healing is gradual; full benefit may develop over 4–8 weeks as inflammation resolves and the nerve recovers. Studies show that well-selected patients experience meaningful improvement in both pain and function. Physical therapy is typically recommended during recovery to strengthen supporting muscles and optimize long-term outcomes.
Frequently Asked Questions
Q: How is this different from open disc surgery (microdiscectomy)?
A: Open microdiscectomy requires an incision, removal of tissue to access the disc, and a longer recovery. Percutaneous disc decompression uses only a needle-sized entry point, preserves surrounding structures, and allows for a much faster return to daily activities — though it is appropriate for a more limited set of patients than open surgery.
Q: What if the procedure does not work?
A: If percutaneous disc decompression does not provide adequate relief, surgical options such as microdiscectomy or fusion remain available. The procedure does not eliminate other treatment options.
Q: Is the procedure covered by insurance?
A: Coverage varies by insurer and technique used. Our team will verify your benefits prior to the procedure and discuss any out-of-pocket costs with you.